Posterior Stabilized Total Knee
Contents:
- The function of the cruciate ligaments
- Posterior stabilized total knee
- The post and cam system
- The results
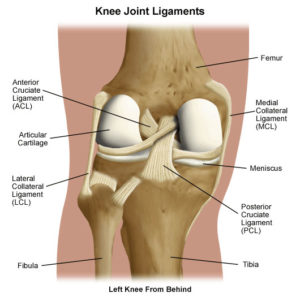
The function of the cruciate ligaments
Inside a healthy knee joint there are two cruciate ligaments. These ligaments, thick as a pencil, are very important to keep the knee joint stable during bending.
In knee joints affected by osteoarthritis and rheumatoid arthritis so much that they need replacement with a total knee prosthesis, the cruciate ligament that lies in front (anterior cruciate ligament) is usually damaged by the disease process and without function. The surgeons remove the anterior cruciate ligament routinely during the total knee replacement operation. Total knee prosthesis functions well even without the anterior cruciate ligament.
After removal of the anterior cruciate ligament there remains the back (posterior) cruciate ligament, usually at first sight still well preserved. The surgeon is now faced with a challenge: remove it or preserve it. That is an enigma.
The posterior cruciate ligament (PCL)
The posterior cruciate ligament (PCL) is a very important stabilizer of the normal knee joint.
The function of the posterior cruciate ligament (PCL) in a healthy knee joint
Click on the icon for a full size picture
When the normal knee joint bends the PCL pulls the upper part of the knee joint – the femoral condyles – backwards. The surgeons call this movement for “rollback”.
(The cruciate ligaments are placed in the middle of the knee joint, so the schematic picture demonstrates a midline section through the knee joint).
Observations on knee joints damaged at accidents demonstrate that in the knee joint with damaged PCL the femoral condyle glides unrestricted forwards during bending. This uncontrolled glide causes severe instability of the knee joint.
In analogy with healthy knee joints, the majority of surgeons believe that PCL exercises similar “roll-back” function in a total knee joint.

(The cruciate ligaments are placed in the middle of the knee joint, so the schematic picture demonstrates a midline section through the upper (femoral) component)
The theory goes as follows:
Stable total knee = total knee with retained posterior cruciate ligament (PCL)
In a total knee joint with retained PCL, the retained PCL “rolls” the femoral component back when the total knee joint bends. The total knee joint is thus stable. The wear of the polyethylene plate in a stable total knee is minimal.
It follows that retained PCL diminishes the wear of the polyethylene component and thus retention of a PCL diminishes the risk of loosening and failure of the total knee prosthesis.
Note that the tibial plate has a space for the PCL. This is a characteristic of a PCL-retaining total knee model.
Unstable total knee = total knee with absent (destructed) PCL
In a total knee joint without PCL, the femoral metallic component glides forwards and backwards uncontrollably during bending and stretching of the total knee joint. The restraint to prevent this motion, the PCL, is lacking.
Uncontrolled sliding of the femoral (metal) component forwards and backwards on the polyethylene tibial component causes increased wear of the tibial plate.
Increased wear of polyethylene increases the risk of osteolysis around the total knee and eventually increases the risk of a failure of the whole total knee joint.
This is the theory. The proof that this mechanism really works in total knees is, however, contested.
The surgeons are, thus, divided:
- one part claims that the PCL should be retained whenever possible,
- other surgeons argue that PCL structure should be removed even if it is intact.
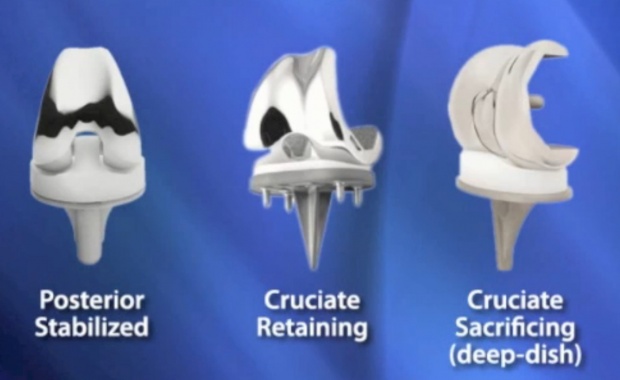
For the patients and surgeons who wish to retain the PCL the manufacturers developed PCL-retaining total knee prostheses.
Those surgeons who remove routinely PCL developed posterior stabilized total knee prostheses.
Posterior stabilized total knee prostheses
In knee joints with fixed deformity (contracture) the PCL has become too short. During the total knee operation, the surgeon is then forced to strip or remove (“sacrifice”) the PCL for correction of the deformity.
Moreover, in knee joints with more severe grades of osteoarthritis, the PCL are severely damaged and without function.
It is common belief among the surgeons that knee joints with damaged or absent PCL cannot be replaced with the conventional total knee prosthesis, such replacement would produce an unstable total knee joint.
For replacement of knee joints without PCL there are thus available special posterior stabilized total knee prostheses.
The stabilization of the total knee joint in these prostheses is achieved by a clever “cam and post” mechanism added to the prosthesis components. This mechanism replaces the function of the PCL.
The principle of a posterior stabilized total knee prosthesis.
The principle of the roll-back mechanism: The tibial polyethylene plate has a central polyethylene post placed on the middle of the plate. In the assembled total knee, the cylindical cam comes against the post when the total knee bends. The post then forces the cam backwards.
In the assembled total knee the tibial post sticks through an opening in the femoral component. When the prosthesis is in place, the post engages the transverse cam. The post and the cam make together a loose transverse hinge. As the total knee bends, this hinge prevents the forwards glide of femoral component, the knee prosthesis rotates around this hinge instead. The post “rolls” the femoral component backwards.
In this way the posterior stabilized total knee replaces the function of the PCL.
Posterior stabilized total knee
There are patients with knee joints damaged by osteoarthritis that are without greater deformity and have a still retained PCL. Yet, many surgeons remove the still retained PCL and use a posterior stabilized total knee prosthesis for replacement of these knees too.
The reason is that the surgeon may have difficulty to balance the retained PCL with the new total joint prosthesis. The PCL is adapted to the natural tibial surface, and not to the tibial plate of the total knee prosthesis.
It is usually easier to put a posterior stabilized total knee prosthesis in a knee joint with removed PCL and get a good stability of the new joint than it is to put a conventional total knee prosthesis in a knee joint with retained PCL and get a stable total knee joint.
The advantages of a posterior stabilized total knees are:
- technically easier to insert
- easier removal of contractures
- less pressure on the polyethylene plate
- better range of motion in the previously stiff knee joint
Disadvantages of a posterior stabilized total knees are
- with unbalanced soft tissues there is a risk of subluxation of the total knee joint
- the post is made of polyethylene and wears off. “Severe” wear of the post was found in about 30 % of all posterior stabilized total knees
- failure of the posterior stabilized total knee caused by wear and damage of the polyethylene post was observed in 3 % of posterior stabilized total knees in a five year observation period according to some reports
- more problem with kneecap (patella). In some reports about 7% patellar fractures, but not all fractures needed treatment. (Thadani 2000)
The results
The debate is still ongoing whether the posterior stabilized total total knee prostheses produce better results than the total knee prostheses with retained posterior cruciate ligament.
As usually, individual studies report widely divergent results.
Some studies demonstrated that the pain relief, return to daily activities, and sense of well being were equal after operations with both types of total knee prostheses. Other studies, however, claimed that patients with posterior stabilized total knee have had better range of motion in the total knee, better stair climbing ability, better walking ability, and less anterior knee pain. (Archibeck 2002)
The Table shows ten year results of two patients groups. The first group had a posterior stabilized total knee, the second group had a total knee model with retained posterior cruciate ligament. (Laskin 2001)
| RESULTS | POSTERIOR STABILIZED | CRUCIATE RETAINING |
| Pain relief excellent | 96 % | 96 % |
| Maximal bending | 114 degrees | 117 degrees |
| Excellent and good results | 98 % | 96 % |
| X-ray lucencies | 2% | 12 % |
| Still in function after 10 years | 97% | 96% |
References:
- Archibeck MJ et White RE J Bone Joint Surgery-Am 2002; 84-A: 1719 – 26
- Laskin RS Clin Orthop 2001; 388: 95-102
- Thadani PJ et al Clin Orthop 2000; 380: 17-29